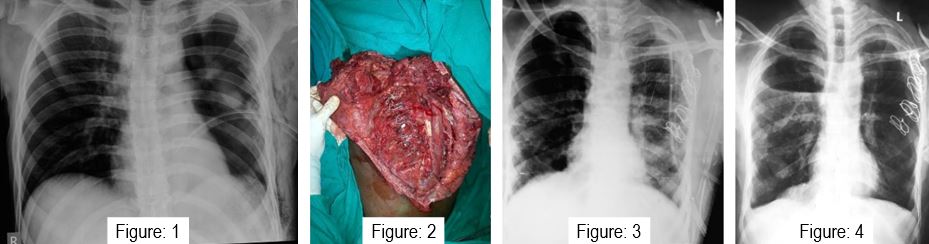
Unilateral flail chest with scapular winging treated with tension band wirings of ribs: A case report
Tanwar M1, Kundu Z S2*, Vashisht G3
1 Tanwar M, Department of Orthopaedics, PGIMS, Rohtak, Haryana, India.
2* Kundu Z S, Professor, Department of Orthopaedics, PGIMS, Rohtak, Haryana, India.
3 Vashisht G, Department of Orthopaedics, PGIMS, Rohtak, Haryana, India.
Tension band wiring is becoming increasingly popular method for stabilizing a flail chest resulting from multiple rib fractures. The indications for fixation of flail chest injuries remain controversial mostly because of a lack of adequate studies [1]. Recent guidelines recommend surgical stabilization of a flail chest based on consistent evidence of its efficacy and lack of major safety concerns. But complications of this procedure can occur and are wide ranging [2]. We report an interesting case of a patient who underwent fixation with tension band wiring for multiple unilateral rib fractures that successfully healed with good functional outcome.
Keywords: Unilateral flail, Tension, Tension
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Orthopaedics, PGIMS, Rohtak, Haryana, India. Email:  |
Tanwar M, Kundu Z S, Vashisht G, Unilateral flail chest with scapular winging treated with tension band wirings of ribs: A case report. ojmpc. 2016;22(1):44-46. Available From https://ojmpc.com/index.php/ojmpc/article/view/28 |
 |