Complications of uncemented total hip replacement in avascular necrosis head of femur, encountered intra and post-operative period
Dwivedi VM1*, Singh V2, Agrawal A3
DOI:Total hip replacement
1* Dwivedi VM, Resident, Department of Orthopaedics, RD Gardi Medical College, Ujjain, MP, India.
2 Singh V, Department of Orthopaedics, RD Gardi Medical College, Ujjain, MP, India.
3 Agrawal A, Department of Orthopaedics, RD Gardi Medical College, Ujjain, MP, India.
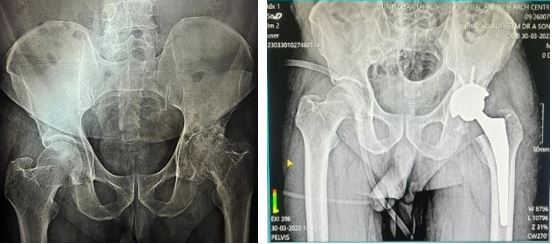
Introduction: Avascular Necrosis Head of Femur is a progressive disorder in which lack of sufficient blood supply leads to cell death, fracture and collapse of the affected area. In stage 3 and 4 patients of AVN of hip, uncemented total hip replacement is the treatment of Choice. The complications in uncemented THR can be intraoperative, postoperative and anaesthetic and also according to time duration can be immediate, early and late.
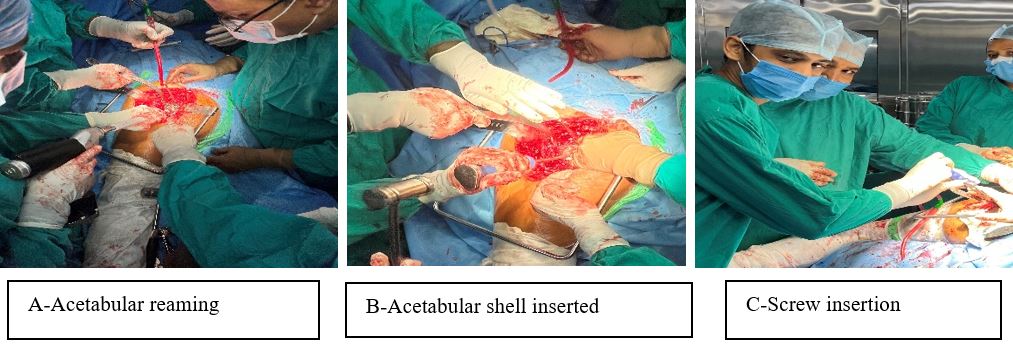
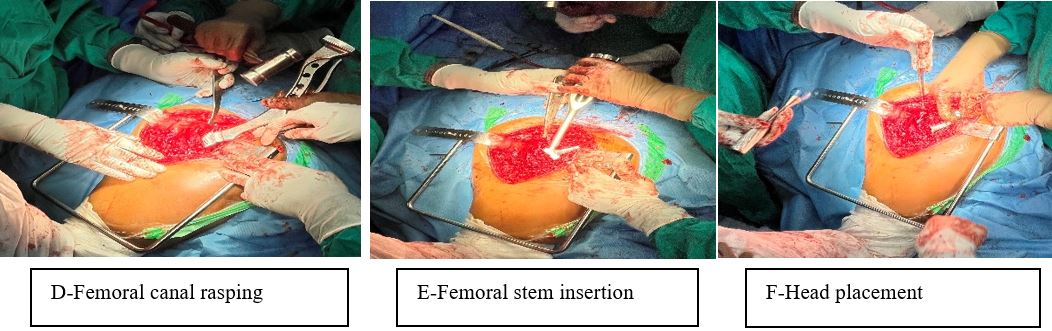
Material and Method: Fifty-one patients of Avascular necrosis of femoral head of stage III and IV, are operated in last two years by uncemented total hip arthroplasty and their results were assessed by Harris hip score. There are few complications which we encountered in intraoperative and post operative period. The assessment and corresponding solutions of the complications are provided in this study.
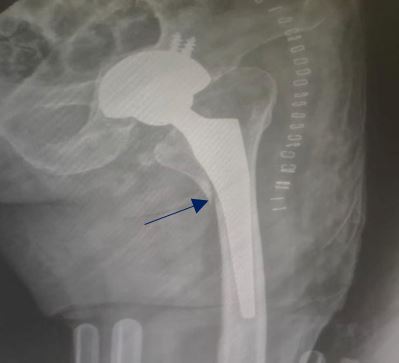
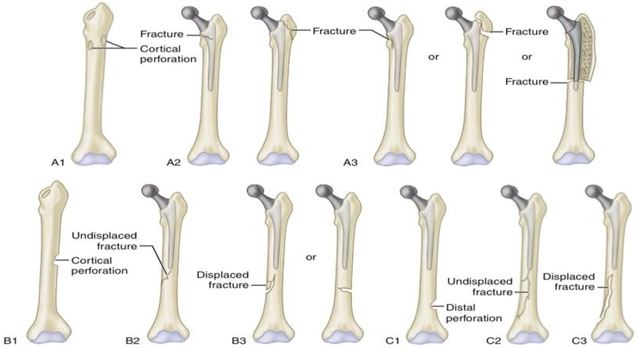
Results: The pre-operative modified harris hip score had a mean of 48.51 with a standard deviation of 3.114. The post-operative modified harris hip score increased significantly to a mean of 90.96 with a standard deviation of 3.268. Intraoperative complication like periprosthetic fracture was seen in 3.9% cases only. The majority (92.2%) did not experience any anesthetic complications. Among those who did, 3.9% encountered hypotension and tachycardia, while 2% experienced postoperative nausea and vomiting. Additionally, one patient (2%) suffered from a spinal headache (PDPH). Post-operative complications were present i.e. 5.9% of the patients experienced sciatic nerve injury, and another 5.9% had superficial infections. Additionally, anterior thigh pain, deep infection, and limb length discrepancy each affected 3.9% of the patients, while 2% experienced dislocation.
Conclusion: Uncemented THR is one of the most successful operative procedure done across the globe. The best possible outcome in uncemented total hip replacement surgery can be achieved by appropriate patient selection, appropriate implant size and design, and above all maintaining sterility intra-operatively and during regular dressings and during suture removal.
Keywords: Uncemented THR, AVN Hip, Complications
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of Orthopaedics, RD Gardi Medical College, Ujjain, MP, India. Email:  |
Dwivedi VM, Singh V, Agrawal A, Complications of uncemented total hip replacement in avascular necrosis head of femur, encountered intra and post-operative period. ojmpc. 2024;30(2):43-49. Available From https://ojmpc.com/index.php/ojmpc/article/view/191 |
 |