Lipoma of bone is a benign neoplasm of adipocytes that typically arises within the medullary cavity of bone. Although there is a large amount of fatty tissue in bone marrow, intraosseous lipoma occurs very rarely, with a 0.1-2.1% prevalence [1-3]. However, this probably is not the actual incidence number because the lesions are frequently asymptomatic. Calcaneus bone is reported to be the most frequent site of intraosseous lipoma [4]. Herein, we present a case of a rare calcaneal intraosseous lipoma.
CASE PRESENTATION
A 47-year-old female patient presented with pain of approx. 6 months duration in the left heel (Figure1). The patient complained of pain on palpation of the medial aspect of the heel and hind foot. The pain increased on weight bearing and shoe contact and subsided with rest. There is no history of focal trauma, and the patient denied any pre-existing inflammatory conditions such as RA, or other metabolic disorders. The patient had been previously treated with NSAIDS with partial relief, but the pain continued.

Figure 1: Left foot lateral x-ray radiograph showing a well-defined, osteolytic lesion in the anterior portion of the body of the calcaneus, with a centralized radiodensity.
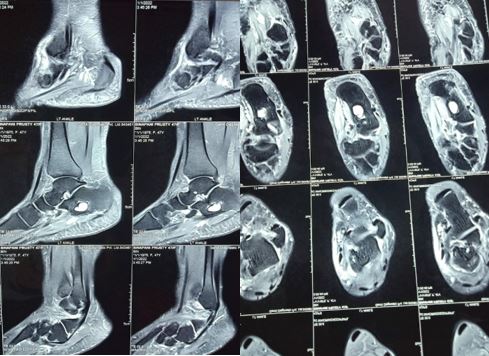
Figure 2: MRI study of the Left ankle; small calcaneal lipoma (measuring ~ 1.7*1.2*1.0 cm).
Her medical history was unremarkable, and the physical examination was only significant for tenderness and edema localized to the medial aspect of the right heel. The range of motion of the ankle was normal;. Laboratory findings, including a complete blood count with differential cell count, erythrocyte sedimentation rate, C-reactive protein, and a biochemical profile that included serum alkaline phosphatase, calcium and phosphate levels were all in the normal range.
Initially a Xray of left foot advised, showing a well-defined, osteolytic lesion in the anterior portion of body of calcaneus, with a centralized radiodensity. A Non-contrast MRI shows small calcaneal lipoma (measuring ~ 1.7*1.2*1.0 cm) (Fig 2). According to Milgram's classification, lesion was graded as a stage 3 calcaneal lipoma because of necrosis, centrally cystic transformed areas and sclerosis in wall. Under aseptic precaution intralesional steroid injection (methyl prednisolone) applied and patient follow up done for 6 months. The result shows good functional outcome. Patient relieved from pain.
DISCUSSION
Intraosseous lipomas, which occur in both males and females, are present in fourth and fifth decades, with a prevalence of 0.1-2.1%. However, real prevalence is thought to be higher than this estimate because most cases are asymptomatic [2,3]. Therefore, most cases have been detected incidentally. Pain is major complication in symptomatic patients, and they present with pathological fractures.
Although intraosseous lipoma can occur anywhere in the skeletal system, 71% of these lipomas are in the lower extremities, and usually appears in the calcaneus (32%), in which the most frequently found tumor is also the intraosseous lipoma. The upper extremities, skull, mandible, and spine are involved with decreasing frequencies. Intraosseous lipomas located in long bones usually affect the metaphysis [5-8]. Basically, simple bone cysts called intraosseous ganglia are present in intraosseous lipomas. On X-rays, intraosseous lipomas appear as benign, osteolytic lesions with well-defined limits, and it is difficult to identify them only based on X-ray findings. Computerized tomography (CT), especially MRI, is useful in differential diagnosis. Radiographic diagnosis of a lipoma may not be straightforward and so there may be differential diagnosis that may include simple bone cyst, nonossifying fibroma, aneurysmal bone cyst, fibrous dysplasia, bone infarct, giant cell tumor, chondroid tumor or fungal infections. The appearance of these lesions on radiographs, CT scans and MRIs can vary as result of their degree of involution and necrosis. It is important to make a correct diagnosis based on multi-method imaging studies, especially MRI.
In classifications performed by Milgram et al. [4], intraosseous lipomas are divided into three stages based on fat necrosis: Stage 1A- sharply limited lesion with homogenous fat content; Stage 2- Dominantly fatty lesions with central necrosis, calcification, or ossification, and Stage 3- A heterogeneous, fat- containing lesion involving multiple necrotic areas, cystic transformations, sclerosis, or ossification in wall. Our case was staged as 3 according to this classification.


