
Uncemented Total Hip Replacement with impaction bone grafting in Protrusio Acetabuli in AVN hip
Singh V1*, Jain P2, Bhinde S3, Agrawal A4
1* Vivek Singh, Professor, Department of Orthopaedics, R D Gardi Medical College and CRG Hospital and Associated Charitable Hospital, Ujjain, Mp, India.
2 P Jain, Department of Orthopaedics, R D Gardi Medical College and CRG Hospital and Associated Charitable Hospital, Ujjain, Mp, India.
3 S Bhinde, Department of Orthopaedics, R D Gardi Medical College and CRG Hospital and Associated Charitable Hospital, Ujjain, Mp, India.
4 A Agrawal, Department of Orthopaedics, R D Gardi Medical College and CRG Hospital and Associated Charitable Hospital, Ujjain, Mp, India.
Background and Aim: Protrusio acetabuli is a central acetabular defect resulting from migration of femoral head medial to Kohler’s line. Idiopathic central displacement of femoral head within the acetabulum is quite rare. However, it may be seen in arthritic hips secondary to rheumatoid arthritis, ankylosing spondylitis, previous trauma, osteomalacia, etc. Primary Total Hip Replacement (THR) in such cases is difficult because of the deficient medial bone, decreased peripheral bony support to the acetabular component and proximal and medial migration of the joint centre. Several techniques described previously in the surgical management of protrusio acetabuli include cemented acetabular components with cement alone or in association with morselized bone graft to reconstruct the acetabulum. However, cement has high rates of migration and loosening of cemented acetabular components in young patients leads to more revision surgeries within the first decade of implantation. The purpose of the study is to describe the technique and results of using impacted morselized bone graft with a porous coated cementless acetabular component in patients with protrusio acetabuli.
Material and methods: A total of 20 primary THR’s (10 unilateral and 5 bilateral) in 15 patients (8 females and 7 males) with protrusio acetabuli were performed between 2018 and 2022, out of which 4 had mild,7 had moderate and 9 had a severe grade of protrusion.
Results: A total of 10 hips were affected by rheumatoid arthritis, 3 by ankylosing spondylitis and 7 had unknown etiology. After the surgery, all bone grafts had united by the sixth month with no perceptible change in acetabular component position in any case. The mean preoperative Harris Hip Score was 48 which improved to 90 at the latest follow-up10 hips (50%) had excellent,8 hips (40%) had good, and 2 hips (10%) had fair results. There was no dislocation.
Conclusion: The use of impacted morselized autograft with a cementless porous acetabular component is a good technique of restoration of hip biomechanics and sound fixation in cases of protrusio acetabuli.
Keywords: Protrusio Acetabuli, Morselised Bone Graft, Uncemented Total Hip Replacement
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor, Department of Orthopaedics, R D Gardi Medical College and CRG Hospital and Associated Charitable Hospital, Ujjain, Mp, India. Email:  |
Singh V, Jain P, Bhinde S, Agrawal A, Uncemented Total Hip Replacement with impaction bone grafting in Protrusio Acetabuli in AVN hip. ojmpc. 2022;28(2):60-64. Available From https://ojmpc.com/index.php/ojmpc/article/view/160 |
 |

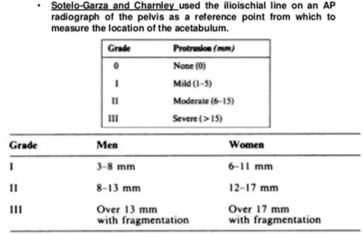


 Figure : 9,10 and 11 One year follow up
Figure : 9,10 and 11 One year follow up