Comparative Evaluation of the Efficacy of Platelet Rich Plasma Versus Triamcinolone in Treating Tennis elbow
Goyal PK1*, Bansal A2, Zuber M3
1* Pratush K Goyal, Senior Resident, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
2 A Bansal, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
3 M Zuber, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
Background: Lateral epicondylitis is seen more commonly in non-athletes than athletes. Non-operative methods are the mainstay of treatment being effective in more than 95% of cases. Platelet rich plasma (PRP) has shown promising results in many studies as compared to steroid injection & other modes of conservative management. Hence, this study was done to compare the efficacy of PRP and triamcinolone injection in management of tennis elbow.
Material and Methods: This randomized study was conducted at our center, for a period of two years from Aug 2015 to Sep 2017 on 60 consenting patients diagnosed as lateral epicondylitis. Patients were randomized into Group –1 (30 patients) receiving 2 ml of PRP injection and group –2 (30 patients) receiving 2 ml of Triamcinolone injection. Post therapy assessment was done using with Oxford elbow score.
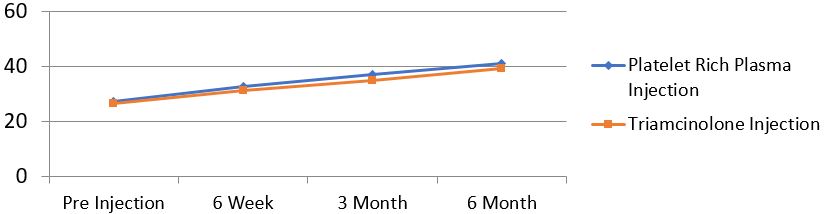
Results: Average age at presentation was 31.11 year (range 20 to 40). Mean Oxford Elbow Score for both PRP injection group and in triamcinolone group at 6 weeks, 3 month and 6 month improved from pre injection score with p-value less than 0.001. On comparing PRP with triamcinolone, PRP was slight better than the triamcinolone injection and results were better maintained for long term in PRP group.
Conclusion: Lateral epicondylitis or tennis elbow is a painful debilitating condition of elbow, which creates disturbance in functional activities. A single injection of PRP at the site of the elbow pain resulted in relief of pain in patients for longer duration as compared to local steroids or other conservative treatments.
Keywords: Tennis elbow, Platelet rich plasma, Triamcinolone, Lateral epicondylitis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India. Email:  |
Goyal PK, Bansal A, Zuber M, Comparative Evaluation of the Efficacy of Platelet Rich Plasma Versus Triamcinolone in Treating Tennis elbow. ojmpc. 2019;25(2):72-76. Available From https://ojmpc.com/index.php/ojmpc/article/view/87 |
 |