Role of Self Help in traumatic dorsolumber spinal cord injury: A case report
Sharma ANK1*, Gohiya A2, Gaur S3
1* Ambica N K Sharma, Resident, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
2 A Gohiya, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
3 S Gaur, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
Introduction: Post traumatic dorsolumbar fractures with spinal cord injuries are always considered a challenging task for any orthopaedician. The degree of functional impairment and health related quality of life (HRQL) depend upon level and completeness of lesion. Physiotherapy and rehabilitation are the keys to make the patient return back to pre-injury status
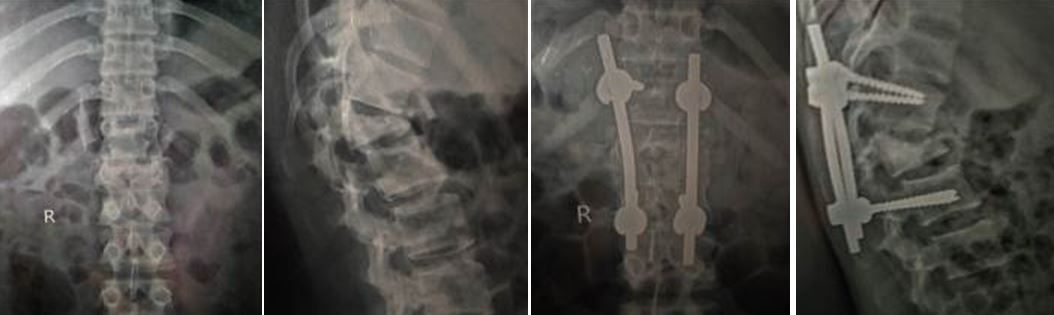
Case Report: Two patients of Dorsolumber spinal injury with almost similar lesion were operated on same day with contrasting outcome.
Conclusion: Role of physiotherapy and rehabilitation cannot be ignored, but a very important aspect of success was self-help.
Keywords: Paraplegia, Spinal Injury, Physiotherapy
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of Orthopaedics, Gandhi Medical College, Bhopal, Madhya Pradesh, India. Email:  |
Sharma ANK, Gohiya A, Gaur S, Role of Self Help in traumatic dorsolumber spinal cord injury: A case report. ojmpc. 2017;23(2):38-40. Available From https://ojmpc.com/index.php/ojmpc/article/view/58 |
 |