Assessment of impact of patient’s age at presentation and Pirani score on treatment duration in clubfoot
Singh VB1, Chaurasia AK2*, Lakhtakia PK3
1 V B Singh, department of orthopedics, S. S. Medical College, Rewa, Madhya Pradesh, India.
2* Amit K Chaurasia, department of orthopedics, S. S. Medical College, Rewa, Madhya Pradesh, India.
3 P K Lakhtakia, department of orthopedics, S. S. Medical College, Rewa, Madhya Pradesh, India.
Background: Delayed presentation of clubfoot is the primary problem in developing nations like India. The purpose of this study was to find out whether the delay in presentation of club feet and its initial Pirani score in infants adversely affect treatment course in terms of number of plaster casts required to achieve complete correction.
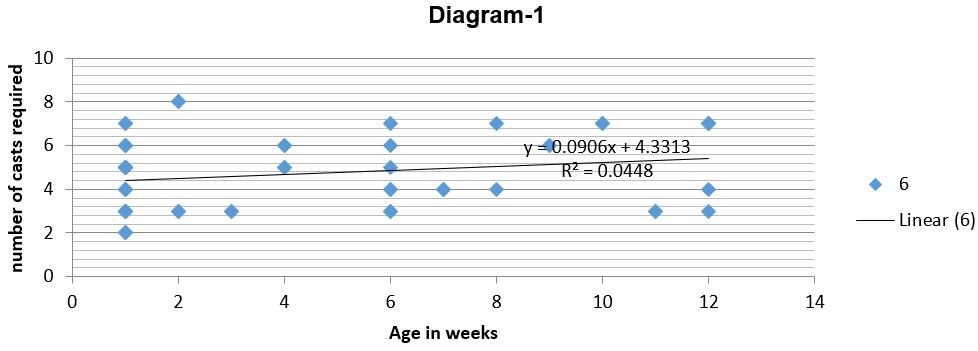
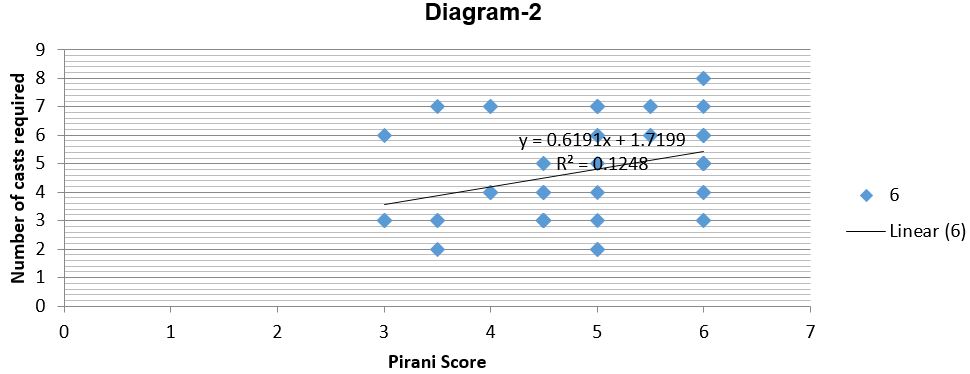
Methods: We retrospectively studied 2 years record of infants with idiopathic clubfoot treated with the Ponseti method. Karl Pearson correlation coefficient (r) was used to find out correlation of patient`s age in months with number of casts required to achieve full correction. We also used this correlation coefficient to find out correlation between severity score of foot and number of casts needed. Correlation was considered statistically significant if P < 0.05.
Results: There was a positive and strong correlation between severity score of foot and number of plaster casts required to achieve full correction and it was statistically significant. We also found a positive but weak correlation between patient`s age in months and number of casts required and the correlation was not found statistically significant.
Conclusion: The number of casts required for correction in idiopathic clubfoot in infant was significantly influenced by its initial Pirani score. However, Age at presentation does not have statistically significant impact on number of Ponseti cast required for correction.
Keywords: CTEV, Ponseti Cast, clubfoot
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , department of orthopedics, S. S. Medical College, Rewa, Madhya Pradesh, India. Email:  |
Singh VB, Chaurasia AK, Lakhtakia PK, Assessment of impact of patient’s age at presentation and Pirani score on treatment duration in clubfoot. ojmpc. 2017;23(2):33-37. Available From https://ojmpc.com/index.php/ojmpc/article/view/57 |
 |