Outcome Following Platelet Rich Plasma Injection In Patients Of Chronic Lateral Epicondylitis
Gupta S1*, Shekhawat YS2, Dhakad T3, Chandrwanshi N4
1* Sameer Gupta, Professor and Head, Department of Orthopaedics, Ja Hospital and GRMedical College, Gwalior, Madhya Pradesh, India.
2 Y S Shekhawat, Department of Orthopaedics, JA Hospital and GRMedical College, Gwalior, Madhya Pradesh, India.
3 T Dhakad, Department of Orthopaedics, JA Hospital and GRMedical College, Gwalior, Madhya Pradesh, India.
4 N Chandrwanshi, Department of Orthopaedics, JA Hospital and GRMedical College, Gwalior, Madhya Pradesh, India.
Background: Various modalities of management are available for lateral epicondylitis which is a common cause of pain around elbow. Many studies have suggested the use of prp (platelet rich plasma) as a safe and effective mode of therapy.
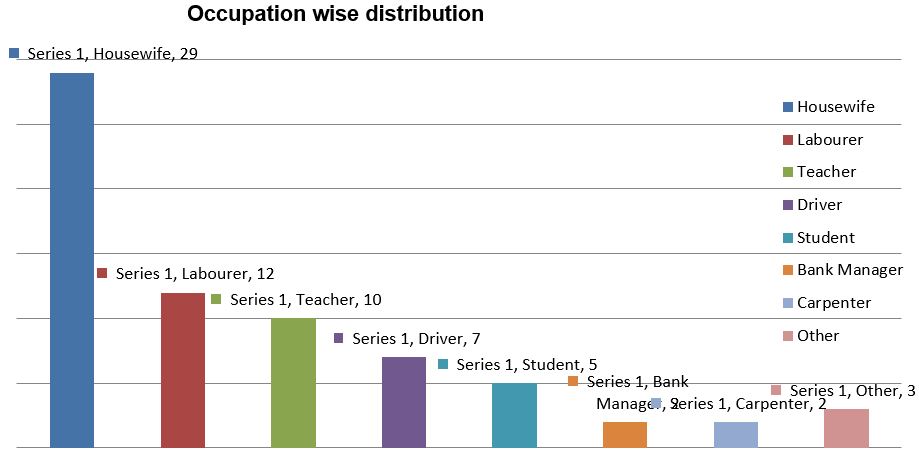
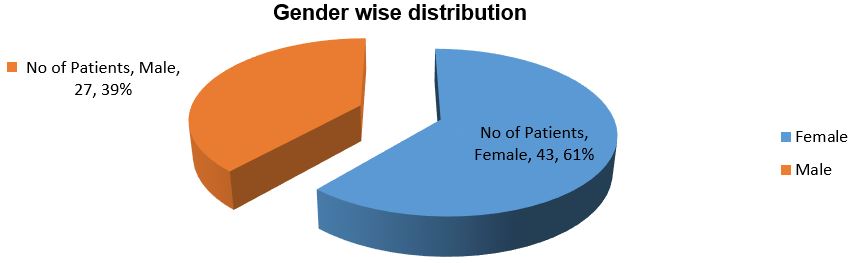
Material and Methods: purpose of this study was to assess the efficacy of prp injection in patients of chronic lateral epicondylitis.It was an interventional study of 70 cases with at least 6 months of symptoms and failed conventional therapy. PRP was prepared from 40 ml autologous venous blood by double centrifugation method.Patients were followed upto 6months. An analysis of result with regards to pain (vas score) was done.
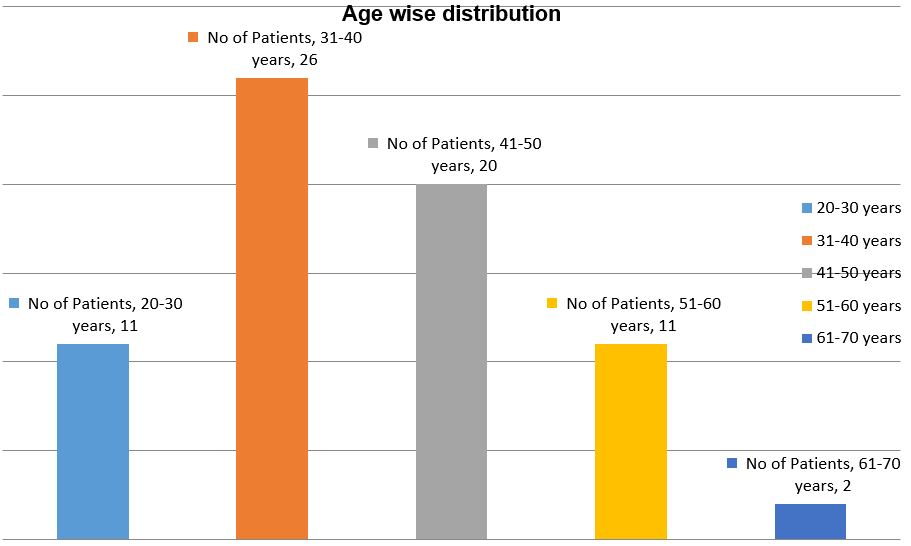
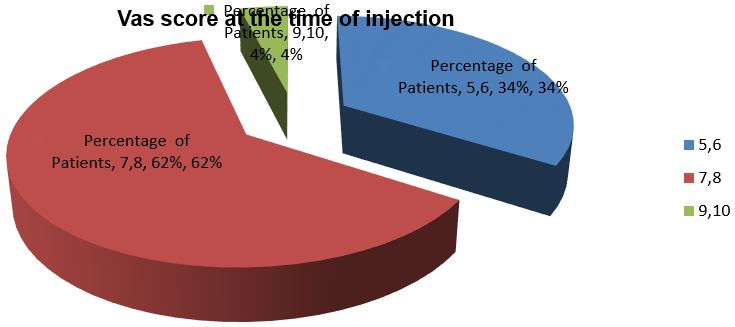
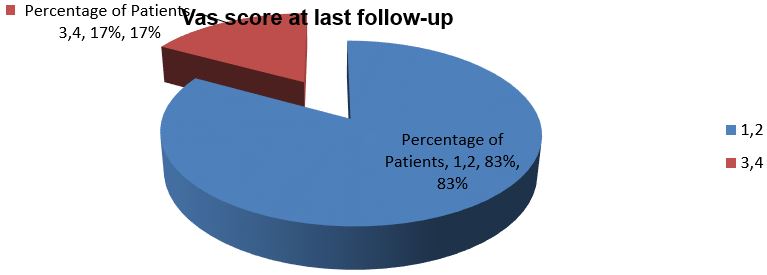
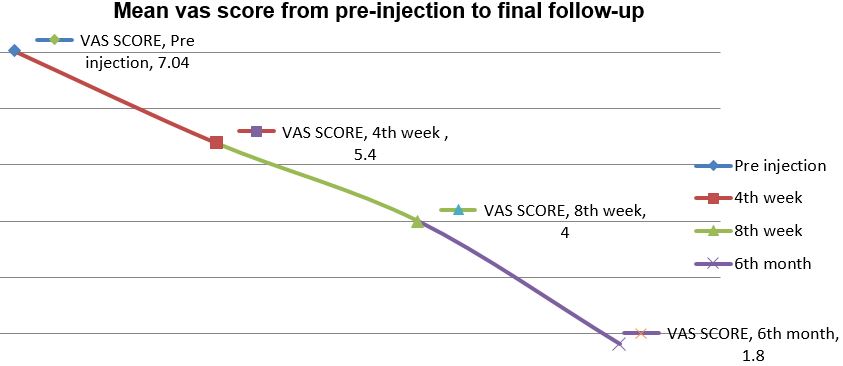
Results: Right elbow was predominantly affected in our sample. Mean age of patients was 41 years. Success was defined as reduction of pain (vas) without re-intervention after a follow up of 6 months. In all patients there was improvement in vas score .pre injection mean vas score of patients was 7.04 and at final follow-up it was 1.84. There was 74 % improvement in vas score. There was progressive improvement with no complications.
Conclusion: Treatment of patients with tennis elbow with prp decreases pain and significantly increases function, even after a follow-up of 6 months.
Keywords: Epicondylitis, Chronic Lateral, platelet rich plasma
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor and Head, Department of Orthopaedics, Ja Hospital and GRMedical College, Gwalior, Madhya Pradesh, India. Email:  |
Gupta S, Shekhawat YS, Dhakad T, Chandrwanshi N, Outcome Following Platelet Rich Plasma Injection In Patients Of Chronic Lateral Epicondylitis. ojmpc. 2017;23(1):12-18. Available From https://ojmpc.com/index.php/ojmpc/article/view/44 |
 |