Centralization of Ulna in Treatment of Giant Cell Tumor of Distal Radius - A Case Report
Jati S1*, Singh P2, Jain N3
1* Jati S, Department of Orthopaedics, Sri Aurobindo Medical College and Post Graduate Institute, Indore, Madhya Pradesh, India.
2 Singh P, Department of Orthopaedics, Sri Aurobindo Medical College and Post Graduate Institute, Indore, Madhya Pradesh, India.
3 Jain N, Department of Orthopaedics, Sri Aurobindo Medical College and Post Graduate Institute, Indore, Madhya Pradesh, India.
Distal end radius is third most common site for Giant Cell Tumour. Various Options for reconstructions are available. In this case report we assessed Functional outcome of centralization of ulna in aggressive giant cell tumour of Distal end radius.
Keywords: Ulna, Distal Radius, Giant Cell Tumor
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Orthopaedics, Sri Aurobindo Medical College and Post Graduate Institute, Indore, Madhya Pradesh, India. Email:  |
Jati S, Singh P, Jain N, Centralization of Ulna in Treatment of Giant Cell Tumor of Distal Radius - A Case Report. ojmpc. 2016;22(2):51-53. Available From https://ojmpc.com/index.php/ojmpc/article/view/40 |
 |
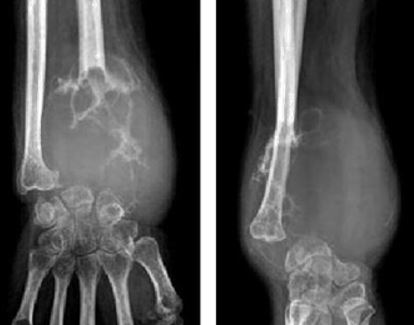
 Figure 1: Clinical Picture
Figure 1: Clinical Picture