Zhu et al.'s study on an urban Chinese population found that road traffic accidents were predominant cause of clavicle fractures in that demographic [13].
Siddharth et al study shows that in total of 62 patients, 42 (67.74%) patients had clavicle fractures from road accidents, 15 (24.19%) from falls, and five(8.06%) from assaults [10].
Saeed Asadollahi et al studied on 134 patients and concluded that most common mechanism of injury was a road traffic accident (78%). Sixty percent (n=83) had an injury severity score of ≥15 indicating major trauma [14].
In a study by Gadegone and Lokhande et al (36 patients), causes of injuries were distributed as follows: 21 cases (58.3%) were due to road traffic accidents (RTA), 12 cases (33.3%) were due to falls, and 3 cases (8.3%) resulted from sports injuries [15].
By Bostmann et al, injury mechanisms included falls from two-wheelers in 38 patients (36.8%), slipping and falling in 24 patients (23.3%), RTAs in 19 patients (18.45%), and sports injuries in 22 patients (21.36%) [16].
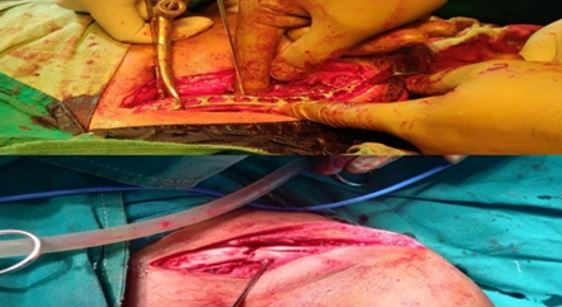
Hartmann et al. reported that 46% of cases were caused by RTAs, 34% by sports injuries, and 20% by falls [17]. In present study TENS group required significantly smaller skin incisions (mean 1.2 cm) compared to CPS group (mean 9.68 cm). This indicates that TENS method is less invasive.
In study by Siddharth et al plating procedure requires large incisions and can injure soft tissues to cause several postoperative complications. Thus, intramedullary fixation (TENs) stands out as a minimally invasive alternative to plate fixation [10].
Meta analysis done by Gao y et al included six randomized controlled trials (RCTs) and nine non-randomized controlled trials (non-RCTs). The study included 513 patients in intramedullary fixation group and 521 patients in plating group. This analysis shows advantage of nailing in small incision site [18].
Pan Hong et al study concluded that ESIN group demonstrated a significantly shorter incision length (2.4 vs. 5.4cm) than plate group (P < 0.001). The SCAR scale was higher in plate than in ESIN group at all time points (P < 0.001), and rate at which cosmetic counsel was sought due to esthetic concerns was also much higher in plate group (71.4%) than in ESIN group (22.2%) (P < 0.001) [11]. In present study duration of surgery was significantly shorter in TENS group (mean 49.77 minutes) compared to CPS group (mean 69.32 minutes). This suggests that TENS procedure is quicker. Blood loss during surgery was significantly less in TENS group (mean 7.95 ml) compared to CPS group (mean 94.55 ml). This highlights less invasive nature of TENS procedure.
Siddharth y et al study concluded that plate fixation had greater intraoperative and postoperative problems than TENs, including more blood loss and more operative time [10].
Meta analysis done by Gao y et al shows less blood loss and less operative time in nailing compare to plating [18].
Pan hong et al, ESIN group demonstrated a significantly shorter operative time (31.1 vs. 59.8min) [11].
Weina Ju et al, Meta-analysis of 1420 records show increased surgical time and soft-tissue stripping with plate fixation [19].
K F Braun et al, Open reduction increases operative time significantly versus closed reduction (open 80.8 ± 35.9 min; closed 30.5 ± 8.5 min) [20].
In present study duration of hospital stay was significantly shorter for TENS group (mean 2.64 days) compared to CPS group (mean 5.05 days). This indicates a quicker recovery for patients treated with TENS method. By vajrangi et al The hospital stay for nailing group (mean 7.95 days) was shorter than that for plating group (mean 9.74 days). This difference was statistically significant (p=0.048) [3].
Pan hong et al ESIN group demonstrated a significantly shorter hospital stay (1.5 vs. 2.5days) [11].
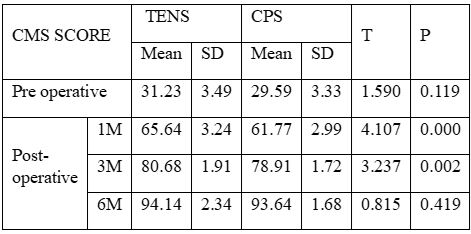
In present study Pre-operative CMS scores were similar between two groups. However, post-operative scores were better in TENS group at 1 month and 3 months. By 6 months, scores were similar between two groups.
Study done by Amit Rahangdale et al research showed that study found that both titanium elastic nails (TENs) and plate fixation have their advantages and disadvantages for treating displaced mid-shaft clavicle fractures. However, choice of surgical method does not significantly impact final functional outcomes measured by DASH and Constant Murley scores [5].
By Siddharth y et al, distribution of scores was very similar between two groups, where 29 (93.55%) patients had an excellent functional outcome. While remaining two patients from CPS group had a good functional outcome, for TENS group, one had a poor, and other had a good functional outcome. During follow-up period of 12 month, Constant-Murley scores were not statistically different between two groups. Still, average score for CPS group (95.45+4.28) was slightly higher than for TENS group (94.19+8.88). deviation of Constant-Murley scores from its average for TENS group (SD=8.88) was twice that of CPS group (SD=4.28) [10].
Jun Sung Park et al done research on 97 patients and conclude that clavicle plate and intramedullary nail (TEN) fixation methods showed very good outcomes in terms of bone union rates and functional scores across all types of clavicle fractures. Patient satisfaction was notably higher with intramedullary nail (TEN) fixation compared to plate fixation [21].
Meta analysis done by Gao y et al shows there were no statistically significant differences found between two groups in terms of shoulder function [18].
Weina Ju et al in their meta-analysis of 1420 records found sufficient data on Constant-Murley scores for meta-analysis were available from 7 studies. Analysis of pooled data of 215 patients undergoing plate fixation and 216 patients undergoing intramedullary fixation revealed no statistically significant difference in Constant-Murley scores between two groups [19].