Introduction
The Hume fracture is an injury of the elbow comprising a fracture of the olecranon with an associated anterior dislocation of the radial head which occurs in children. It was originally described as an undisplaced olecranon fracture, [1] but more recently includes displaced fractures and can be considered a variant of the Monteggia fracture.[2] The injury was described in 1957 by A.C. Hume of the orthopaedic surgery department of St. Bartholomew's Hospital, Rochester.[1]
Although the precise mechanism of injury is unclear, the injury occurs in children who have fallen heavily with their arm trapped under the body. In his original description of the injury, Hume suggested that the injury occurred as a result of hyperextension of the elbow leading to fracture of the olecranon, with pronation of the forearm leading to the radial head dislocation.[1]
In the original description by Hume, where the olecranon fractures were not displaced, treatment consisted of closed reduction of the radial head dislocation under general anaesthesia by supination of the forearm. This was followed by immobilisation of the arm in a plaster cast with the elbow flexed at 90° and the forearm in supination for 6 weeks.[1]
Where the olecranon fracture is displaced, open reduction internal fixation is recommended. Once the olecranon has been repaired, closed reduction of the radial head dislocation is usually possible. This is followed by immobilisation with the elbow flexed to 90° and the forearm in the neutral position. The duration of immobilisation depends on clinical assessment of the joint, and mobilisation may be possible after as little as 4 weeks.[2]
Case report
A 9 years old female presented in our opd with history of trauma due to fall in home 1 month back, with complain of pain and swelling in right elbow with completely extended right elbow and no flexion in elbow for 1 month. Patient was treated by conservatively elsewhere. On examination patient is having tenderness, swelling and completely extended right elbow with no movement at elbow. Diagnosis was Hume fracture-malunited Monteggia Fracture variance, right elbow.
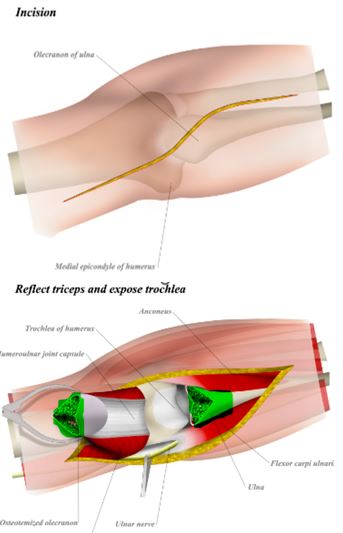
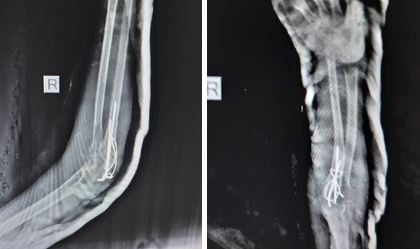
Preoperative profile, x-ray and CT scan of elbow is done and patient is operated by posterior trans-olecranon approach. Olecranon shortening is done by freshened the fracture ends and tension band wiring of olecranon is done. Physiotherapy of elbow started from third post operative day. Patient was followed up regularly. Tension band wiring is removed after five months of surgery because wires are protruding from skin. At 5 months follow up patient is having 90 degree of flexion and 120 degrees of extension from completely extended elbow.

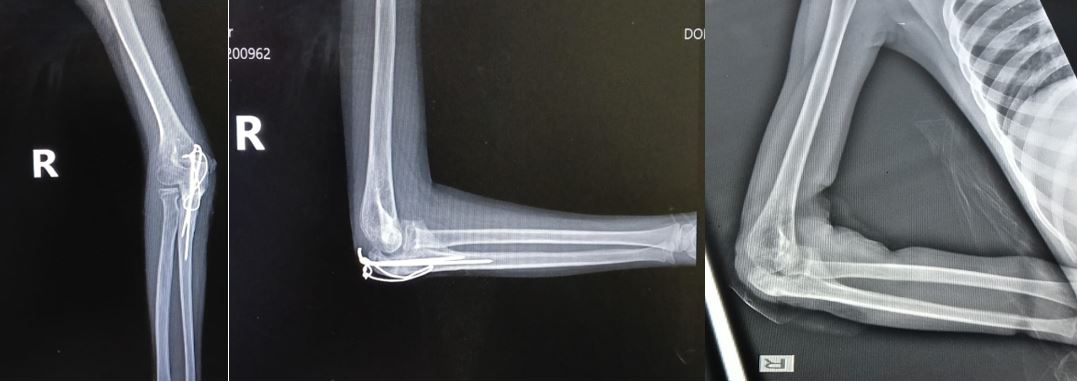
Figure 1: A, B, C, D- Preoperative X-ray and CT scan of patient
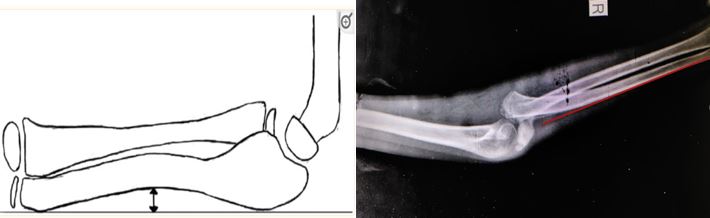
Figure 2: A-The ulnar bow sign- a dorsal line is drawn from olecranon to the distal edge of the ulna on a lateral view, more than 1 mm gap indicates a curvature in the ulna, B- Ulnar bow sign was absent in our case.
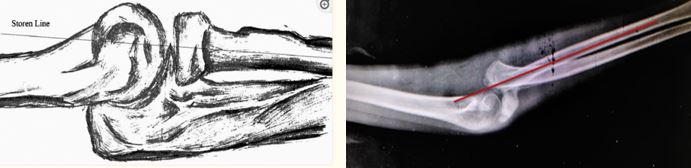
Figure 3: A- Soren line- the axis of radius normally travels through the center of humeral capitellum, in lateral view. B- It was passing anterior to capitellum in our case.
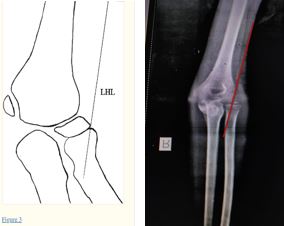
Figure 4: A- The lateral humeral line along the lateral margin of humeral lateral condyle and is parallel to the axis of distal humeral shaft on AP view.