Lateral Extra articular Tenodesis (L.E.T.) to control Anterolateral instability associated with ACL (Anterior cruciate ligament) deficient knees– A Novel study
Dubey A1*
1* Ashish Dubey, Peetambara hospital 29, Nehru colony, Gwalior, Madhya Pradesh, India.
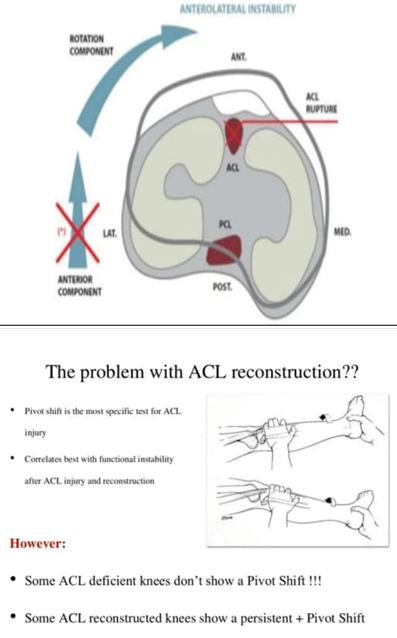
Introduction: Chronic ACL laxity, in particular Rotational laxity associated with an explosive pivot shift test, has being tend to cause combined damage to ACL and Anterolateral structures of knee. We, hereby present a study of adding a LET procedure to such Anterolateral Rotational instability.
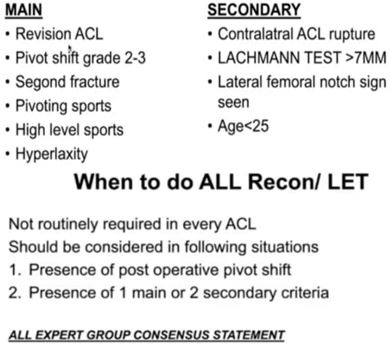
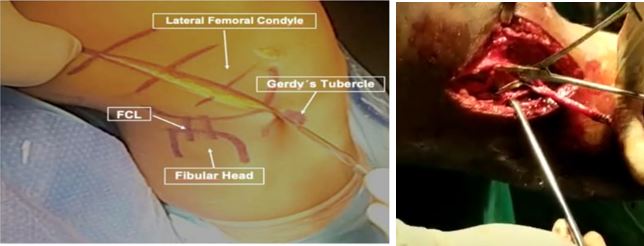
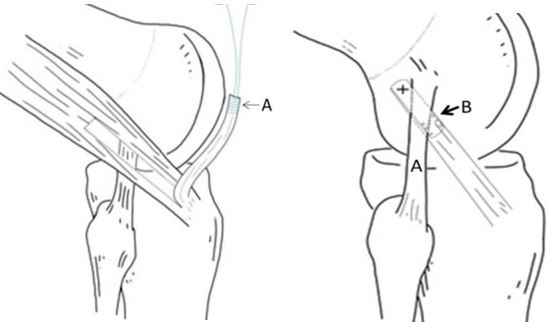
Material and methods: We operated 8 cases (All males) with complete ACL tear with Anterolateral instability (7 patients with Grade 2 Pivot shift test,1 with Chronic ACL injury) from May 2020 to October 2021.We did primary ACL reconstruction in all knees, with adding LET procedure (Modified Lemaire’s technique).
Results: All patients were followed up for period of 6 months to 1 year (Average 8.6 months). A pre & Postoperative outcome scores were assessed by Lachman test, Pivot shift test (-ve in all, in post-op follow-up), Lysholm score (mean 90.75, %,) and Tegner score (average Gr 4).
Conclusion: After this study we can conclude that adding a LET procedure (Modified Lemaire’s technique) to an ACL deficient knee with Anterolateral instability (like explosive Pivot shift test), is beneficial as not only it reduces the Anterolateral instability but also, greatly reduces the risk of Graft Failure.
Keywords: LET procedure, Anterolateral instability, ACL reconstruction
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , , Peetambara hospital 29, Nehru colony, Gwalior, Madhya Pradesh, India. Email:  |
Dubey A, Lateral Extra articular Tenodesis (L.E.T.) to control Anterolateral instability associated with ACL (Anterior cruciate ligament) deficient knees– A Novel study. ojmpc. 2024;30(1):29-33. Available From https://ojmpc.com/index.php/ojmpc/article/view/186 |
 |