Functional outcome of elastic nail fixation for Intertrochanteric fracture in medically high-risk elderly
Tirkey R1, Vidyarthi A2, Rajak CB3*
1 R Tirkey, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
2 A Vidyarthi, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
3* Chandra Babu Rajak, Department of Orthopaedics, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
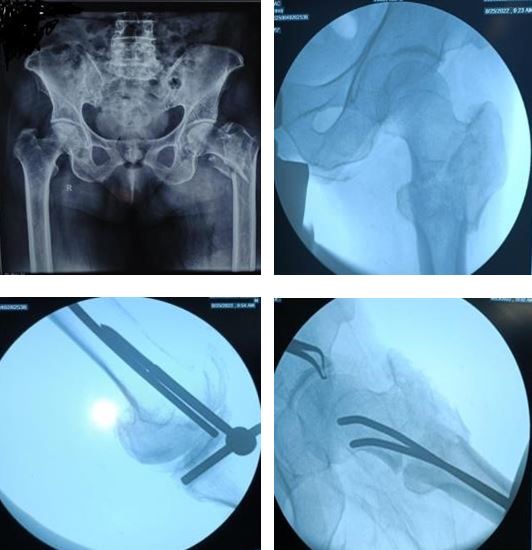
Introduction: Intertrochanteric fractures in elderly population are major health problem. There are so many implants available to treat these fractures. We used enders nail for intertrochanteric fractures in medically compromised and high-risk patients.
Material and method: Twenty-seven patients of intertrochanteric fractures of femur were operated by condylocephalic ender’s nail. We included elderly patient with age more than 60 year with high risk and medically compromised conditions. The clinical and radiographically assessment was done in all cases at 4-week, 6-week, 12 week and 6 months.
Results: Fracture healing was achieved in average 12.5 week (ranging from 10 week to 24 week). The mean Harris score was 82.
Conclusion: Our experience suggests that the chief indication of enders’ nail fixation is in the treatment of intertrochanteric femur fracture in critically ill patient who cannot tolerate anaesthesia for an hour and more. Ender’s nailing appears the least traumatic form of internal fixation.
Keywords: Intertrochanteric femur fractures, enders nailing, old patients
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , , Department of Orthopaedics, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India. Email:  |
Tirkey R, Vidyarthi A, Rajak CB, Functional outcome of elastic nail fixation for Intertrochanteric fracture in medically high-risk elderly. ojmpc. 2024;30(1):17-20. Available From https://ojmpc.com/index.php/ojmpc/article/view/184 |
 |