Missed Monteggia fracture in children- A case series
Khare A1*, Mandlecha P2
1* Ajay Khare, Director, Global Hospital, Ujjain, Madhya Pradesh, India.
2 P Mandlecha, Global Hospital, Ujjain, Madhya Pradesh, India.
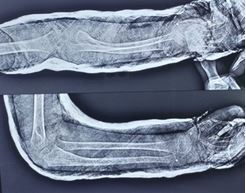
Background: Missed Monteggia fractures in children may cause pain, deformity, decreased range of motion, and neurological symptoms. Various surgical techniques have been advised to reconstruct long-standing Monteggia injuries to get long-term upper limb function. The purpose of this study was to assess the clinical and radiographic results of surgical technique for missed Monteggia fracture-dislocations.
Material and method: A prospective evaluation of 5 patients who underwent surgical reconstruction of missed Monteggia fracture-dislocations was performed. The median patient age at the time of surgery was 10 years, and the median time from injury to surgery was 13 weeks. Median clinical and radiographic follow-up was one year.
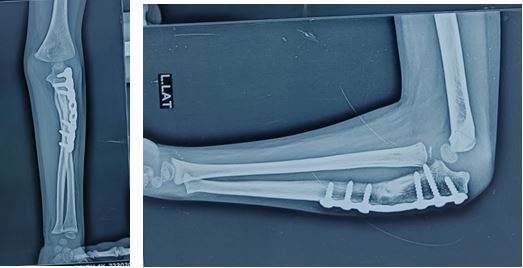
Results: The median elbow range of motion improved from 90 degrees of flexion and 5 degrees short of full extension preoperatively to 120 degrees of flexion and full extension postoperatively. Forearm range of motion also improved from a median of 80 degrees of pronation and 60 degrees of supination preoperatively to 80 degrees of pronation and 80 degrees of supination postoperatively. Congruent radiocapitellar alignment was maintained in 4 patients. One patient had redislocation of the radiocapitellar joint, and 1 patients had radiographic re-subluxation. One of the 5 patients who experienced redislocation underwent early revision and achieved uncomplicated long term result.
Conclusion: Good improvements in elbow motion and radiocapitellar stability can be safely achieved in the majority of children following surgical reconstruction of missed Monteggia lesions.
Keywords: Khare et al. Missed Monteggia fracture in children
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Director, , Global Hospital, Ujjain, Madhya Pradesh, India. Email:  |
Khare A, Mandlecha P, Missed Monteggia fracture in children- A case series. ojmpc. 2024;30(1):12-16. Available From https://ojmpc.com/index.php/ojmpc/article/view/183 |
 |