Introduction
Fracture neck of femur is aptly called as “the unsolved fracture”. This is because even with so much of advances in orthopedic field, there is no simple method of treatment which can give consistently successful results for this fracture. Management of this fracture especially in younger patients is a really demanding and challenging task for any orthopaedic surgeon (1). Fracture neck of femur is common in old people as many of them are osteoporotic. With improvement in quality of life leading to increased life expectancy, the incidence is even more common nowadays. Due to the congested vehicular traffic, it is also commonly seen in young patients after road traffic accidents and many a times they are polytraumatized. Many of these fractures are unstable. Because of its peculiar blood supply, a fracture neck of femur may cause circulatory disturbance leading to avascular necrosis and non-union. So, every fracture neck of femur should be treated as an emergency (2). It should be reduced accurately anatomically and fixed stably by one of the many implants available now. Usually, undisplaced stable fractures have a good prognosis and displaced unstable fractures a poor prognosis.
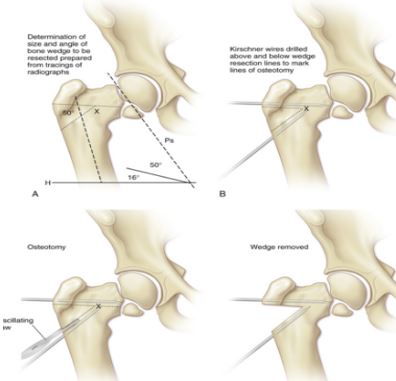
In Madhya Pradesh, because many patients go to native bone setters for treatment of fractures, these patients present with non-union of fracture neck of femur. Another factor leading to non-union is the angle of inclination of fracture. Usually, horizontal fractures with less than 30° of angle unite well and those with more than 30° may result in non-union even when treated expertly (3). This is because in fractures with more than 30° of inclination the resulting forces will act as shearing forces leading to displacement of fragments and non-union. The Pauwels’ principle which was described in 1927 is used, even today successfully. Pseudoarthrosis of femoral neck will unite, if inclination of pseudoarthrosis is changed in such a way that the shearing forces are converted into compression forces and converting unstable fracture into stable one. This leads to endochondral ossification of the fibrocartilage at pseudoarthrosis making the fracture to unite (4). Since, our patients require squatting for their routine daily activities, it is important to preserve the natural femoral head by making the fracture unite. One should not think of prosthetic replacement for every patient with fracture neck of femur. The best end result after fracture neck of femur treatment is the patient’s own healed femoral head and neck and every attempt must be made to achieve that goal (5).
Non-union after femoral neck fracture is defined as lack of radiographic evidence of union 6 months after fracture. King [6], in 1939, in his comprehensive review of both recent and old case of fracture neck femur, emphasized that 3 weeks old can be arbitrarily called old and ununited, as it can be assumed that the head of the femur is devoid of its blood supply, has less chances of osseous union and that secondary changes are more probable, than if operation were performed earlier. If the fracture neck of femur remains untreated for more than 3 weeks, internal fixation alone is likely to have high rate of non-union, as reported by Barnes et al. [1]; in their series on fractures of more than 1-week duration they had non-union rate as high as 50%.
The femoral neck fracture is probably the fracture, for which there exists the larger number of methods of osteosynthesis. Internal fixation of femoral neck fracture is followed by certain incidence of fixation failure. Nonunion may occur in one-third of patients, with higher rate in vertical or displaced fractures [7]. Number of methods of internal fixation when used alone has failed to achieve the desired end result. Osteoporosis directly influences degree of displacement and quality of internal fixation. The deficient bone stock and posterior comminution play a significant role in biological failure to unite the fracture. Age and sex of patient, osteoporosis, degree of displacement and quality of fracture reduction are the factors that have been found to affect the end result [8, 9]. The appropriate treatment for non-union of a femoral neck fracture depends on the age of the patient, his or her medical status, viability of the femoral head, size of the remnant femoral neck, osteoporosis, duration of the disease and finally the state of joint space. In patients younger than 55 years who are in good general medical condition, with no osteoporosis and with a reasonable size of femoral neck and normal joint space, it is desirable to preserve the femoral head, particularly if the patient’s lifestyle and social and religious customs require squatting and sitting in a cross-legged position [10]. Treatment options for femoral neck non-union with preservation of the femoral head include refixation of the fracture, refixation and bone grafting, a pedicle graft to provide blood supply, or a valgus osteotomy with fixation. Cortical bone grafts have been associated with dis-impaction or angulations of the head leading to failure [11]. The initially reported success of Meyer’s procedure has not been reproduced in a large series and the procedure has been considered unreliable [12]. Arthrodesis has a high failure rate but, when successful, it leads to a functional but immobile hip. Different techniques of vascularized bone grafting have been introduced, often with excellent results [13, 14], but the usefulness of these techniques is limited because of donor-site morbidity and limb length discrepancy with residual varus deformity.
We believe, that valgus osteotomy acts as a biological stimulus for healing of these fractures, promoting osteogenesis as a result of conversion of shearing forces to compressive forces across the fracture site. The osteotomy is relatively easy to perform, cost effective, provides stability and often is definitive one-time surgery. Valgus osteotomy and internal fixation with dynamic hip screw and angle barrel plate plays a twofold role, it converts the shearing forces into the compression forces by placing the fracture site perpendicular to the resultant of body weight forces; and it buttresses the head of femur from below to improve stability provided by the internal fixation. Osteosynthesis with dynamic hip screw in its optimum position in the femoral head, supplemented by the buttressing effect of the distal osteotomy fragment, maintains coaptation and immobilization of the fragments and provides a high degree of stability. Following osteotomy, valgus orientation of the proximal femur decreases the lever arm and therefore increases contact pressure on the head. keeping in mind the facts of above-mentioned studies, it seems that performing valgus osteotomy in a hip with changes of AVN may lead to progression of disease and a painful hip later on, and therefore we excluded these patients from our study.