Functional Outcome of Proximal Tibial Sagittal Fractures Treated with Minimally Invasive Plate Osteosynthesis
Jati S1, Bansal H2*, Bohra T3, Kumar M4, Daya M5
1 S Jati, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
2* Himanshu Bansal, Assistant Professor, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
3 T Bohra, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
4 M Kumar, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
5 MJ Daya, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
Background: Tibial plateau fractures are common intra-articular fractures, representing 1-2% of all fractures. Modern locking plate systems provide increased angular stability, have a low implant profile, improved design matching the peri-articular bone surface and are compatible with minimally invasive techniques. We evaluated the functional outcome of tibial plateau sagittal fractures using a locking compression plate done via a minimally invasive technique.
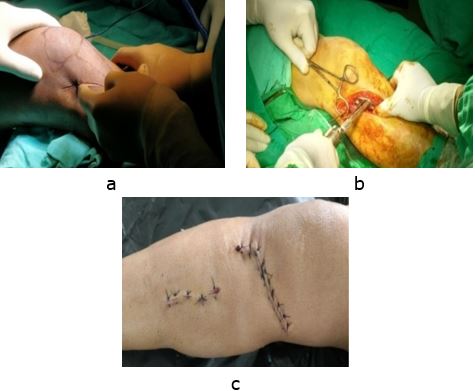
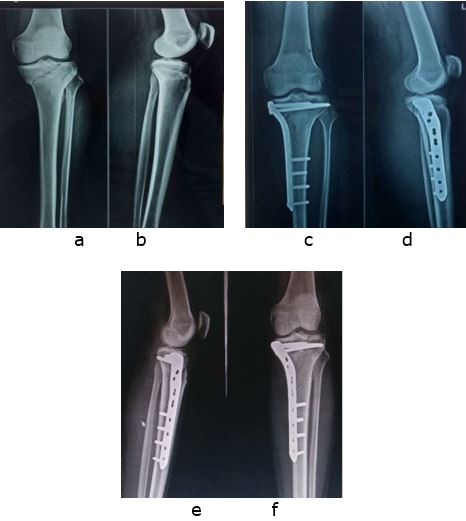
Material and methods: 60 cases of sagittal plane proximal tibial fractures of Schatzker type I, IV, V, and VI fractures were treated using locking compression plate via minimally invasive techniques and were assessed for functional outcome by Modified Rasmussen’s score.
Results: A total of 52 patients with a mean age of 43.71 years were included in the study (8 patients were lost in follow-up). 39 were male and 13 were female. 30 patients (58%) had excellent, 19 patients (36%) had good, 3 patients (6%) had fair functional outcome and none of the patients had a poor outcome. The mean Rasmussen score in the series was 25.85.
Conclusion: Internal fixation of proximal tibial sagittal fractures with locking plates, following the principles of MIPO (Minimally invasive percutaneous osteosynthesis) provides, satisfactory fracture reduction, less damage to soft tissues, allows early mobilization and excellent to good functional outcome even in these complex tibial plateau sagittal fractures.
Keywords: Tibial plateau fracture, Locking compression plate, Proximal tibial fracture
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India. Email:  |
Jati S, Bansal H, Bohra T, Kumar M, Daya M, Functional Outcome of Proximal Tibial Sagittal Fractures Treated with Minimally Invasive Plate Osteosynthesis. ojmpc. 2021;27(2):94-98. Available From https://ojmpc.com/index.php/ojmpc/article/view/136 |
 |