Functional outcome of distal end femur fractures treated by minimally invasive plate osteo-synthesis using locking compression plate: a prospective study in 50 adults
Jati S1, Bansal H2*, Bohra T3, Kumar M4
1 S Jati, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
2* Himanshu Bansal, Assistant Professor, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
3 T Bohra, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
4 M Kumar, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India.
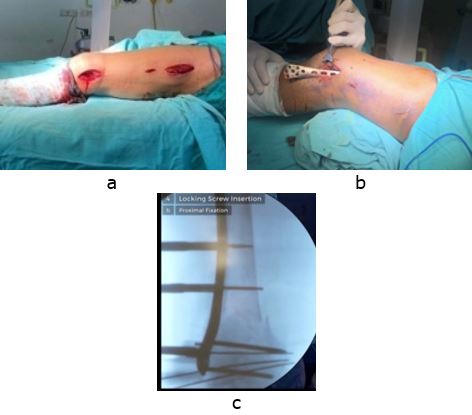
Background: Distal femoral locking compression plate can be done via a minimally invasive method, overcoming the drawbacks of excessive periosteal stripping as caused by the open method. The fixed locking construct of the plate also provides stable fixation needed for early mobilization in fractures of the distal femur. Hence, we evaluated the results of the distal femoral locking compression plate done via minimally invasive technique in fractures of the distal end femur.
Material and methods: 50 cases of fracture distal end femur were treated by internal fixation with distal femoral locking compression plate via minimally invasive techniques and were evaluated radiologically for union and functionally using NEER’S Score.
Results: 50 distal end femoral fractures (29 males and 21 females) with a mean age of 51 years (range 20 to 83 years) were included in the study. The mean duration for surgery was 67 minutes (range 60 to 89 minutes), mean blood loss was 119 ml (range 100 to 140 ml) and mean union time was 14.3 weeks (range 11 to 20 weeks). 38 (76 %) patients had excellent results and 8 (16%) had satisfactory results as per NEER’s scoring system with a mean NEER’s score of 90.133 (range 74 to 96). Complications were knee stiffness as seen in 4 (8%) cases, 4(8%) had a superficial infection, 1 (2%) had implant failure, 2 (4%) had mal-alignment and 1(2%) had nonunion.
Conclusion: Pre-contoured distal femoral locking compression plate by virtue of its features provide stable fixation and done via minimally invasive technique, provides excellent function, high rate of bone union, and fewer complications, even in severely comminuted fractures and osteoporotic bones of distal end femur.
Keywords: Distal end femur fracture, Locking compression plate, Neer’s scoring system, Minimal invasive technique
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Orthopaedics, Sri Aurobindo Medical Science and Post Graduate Institute, Indore, Madhya Pradesh, India. Email:  |
Jati S, Bansal H, Bohra T, Kumar M, Functional outcome of distal end femur fractures treated by minimally invasive plate osteo-synthesis using locking compression plate: a prospective study in 50 adults. ojmpc. 2021;27(2):64-69. Available From https://ojmpc.com/index.php/ojmpc/article/view/134 |
 |